35YEAR OLD MALE WITH SOB
This is an online E log book to discuss our patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patient's problems through series of inputs from available global online community of experts with an aim to solve those patient's clinical problems with collective current best evidence based inputs. This E log book also reflects my patient-centered online learning portfolio and your valuable inputs on the comment box.
CHIEF COMPLAINTS
A 35 year old male who is daily wage worker came with chief complaints of shortness of breath and fever since 1 week.
HISTORY OF PRESENT ILLNESS
Patient was apparently asymptomatic 1 week back, then he developed
• shortness of breath on exertion, since 1 week.
• high-grade fever since 1 week, more during night, relieved on medication and relapses back.
• decreased urine output since 1 week
• dragging type of pain in both legs and hands, associated with generalised weakness.
• No food intake since 1 week
• orthopnea and PND present since 4 days
HISTORY OF PAST ILLNESS
No history of DM, HTN, TB, Epilepsy, leprosy, CAD, CVN, Asthma or any other chronic illness.
No history of previous transfusion.
PERSONAL HISTORY
Built : Weakly nourished
Appetite : Decreased since 1 week
Diet : mixed
Sleep : Decreased since 1 week
Bladder movements:
Anuria since 1 day associated with burning micturition.
Bowel movements: regular
Addictions : toddy consumer in summer season.
Regular alcohol consumer, once a week.
No h/o smoking
FAMILY HISTORY
His wife was diagnosed with pulmonary TB, got admitted in hospital 1 month ago.
GENERAL EXAMINATION
Patient was coherent, cooperative and conscious. Well orientated to time and space.
Pallor : absent
Icterus : absent
Clubbing: absent
Cyanosis : absent
Koilynochia: absent
Pedal edema : absent
Lymphadenopathy: absent.






 Vitals:
Vitals:



















Biphasic T waves in V1 - V4









Temperature:

Blood pressure:110/70mmhg
Respiratory rate:16cpm
Pulse rate:110bpm
SYSTEMIC EXAMINATION
Respiratory system
Inspection
Shape and symmetry of chest : normal, symmetrical
Trachea : central
Respiratory movements: normal
Apical impulse: seen
Skin over the chest : normal
Dysnea : present
Palpation
Trachea : central
Respiratory movements: normal
Fremitus : normal
Percussion
Normal
Auscultation
Breath sounds: vesicular
Adventitious sounds : absent
Vocal resonance: normal on both sides
Other systems
CNS : No facial asymmetry, all reflexes are normal.
GIT : Tenderness present in hypochondrium, umblical and right lumbar region.
Liver and sleep not palpable.
Mild ascites.
CVS : Thrills , present
S1, S2 heard
No murmers.
Raised JVP.
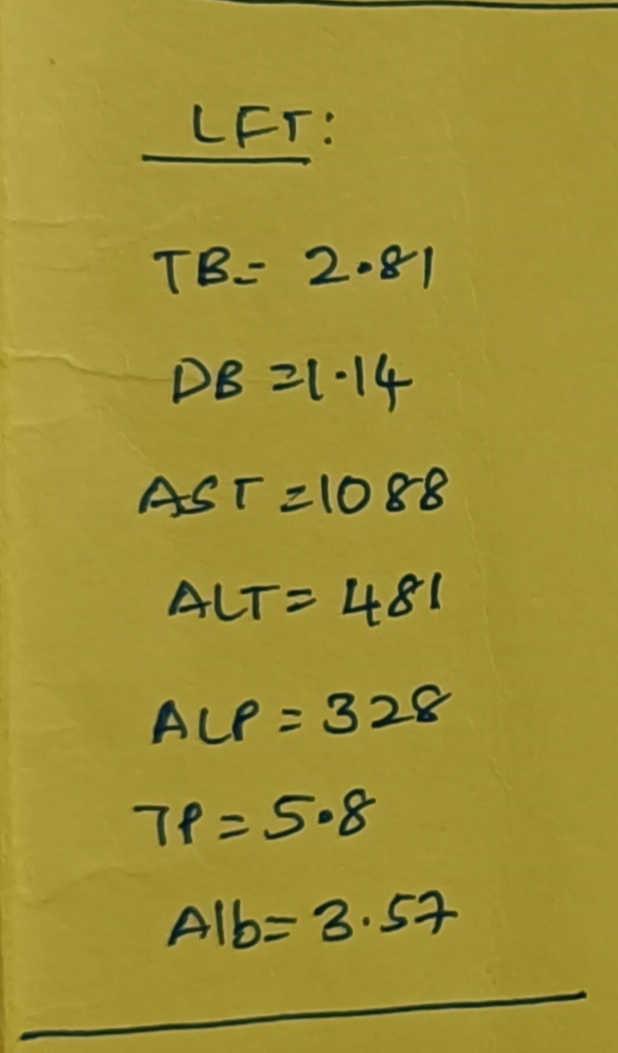
INVESTIGATION:















CHEST X RAY

ABDOMINAL X RAY

ECG FINDINGS:

Biphasic T waves in V1 - V4
T wave inverted in II, III, avf.
2D echo findings:
-D shaped LV
-Severe TR+ with PAH
-Trivial MR+/AR+
-No AS/MS
-EF=60, RSVP=80mmHg
-No diastolic dysfunction
-Minimal PF+
-Dilated RA,RV,IVC
-IVC size(2.0cm)-non collapsing
USG FINDINGS:

PROVISIONAL DIAGNOSIS:
Right heart failure
-Severe pulmonary artery hypertension,
-Type1 respiratory failure(Resolved)
-Edematous bowel loops,
-Prerenal AKI,
-Severe metabolic acidosis 2° to sepsis ?
- Acute hepatitis
TREATMENT:
1)O2 inhalation, increase or decrease according to requirement, spo2>/=92%
2)Neb with DUOLIN 6th hourly
3)INJ.PIPTAZ 2.25gm IV/TID
4)INJ.LASIX 40mg IV/BD
5)IVF NS/RL @50ml/hr/IV
6)INJ.PAN 40mg IV/OD
7)INJ.THIAMINE 200mg in 100ml NS/IV/BD
8)INJ.OPTINEURON in 100ml NS/IV/OD over 30min
9)T.DOM 10mg PO/BD
10)VITALS MONITORING 4TH HOURLY
11) TEMPERATURE MONITORING 4TH HOURLY
12) STRICT I/O MONITORING


Comments
Post a Comment